
Indiana Medicaid Prior Auth Form
Indiana Medicaid Prior Auth Form - Prior authorization is required for certain covered services to document the medical necessity for those. Web see the ihcp provider quick reference at in.gov/medicaid/providers for mailing address or fax number. Check the radio button of the entity that must authorize the service. Web an indiana medicaid prior authorization form is a document used by medical professionals to request medicaid coverage for a prescription drug not. The indiana health coverage programs (ihcp) requires prior authorization (pa) for certain covered. Web covermymeds is envolve pharmacy solutions’ preferred way to receive prior authorization requests. Web this form is for providers to request prior authorization for services covered by indiana health coverage programs (ihcp). Web access the caresource indiana medicaid prior authorization list. (for managed care, check the. Please refer to the procedure code lookup tool to.

20182024 Anthem Member Authorization Form Fill Online, Printable, Fillable, Blank pdfFiller
Please refer to the procedure code lookup tool to. Web see the ihcp provider quick reference at in.gov/medicaid/providers for mailing address or fax number. Web this form is for providers to request prior authorization for services covered by indiana health coverage programs (ihcp). Check the radio button of the entity that must authorize the service. Prior authorization is required for.

Free Alabama Medicaid Prior (Rx) Authorization Form PDF eForms
Web this form is for providers to request prior authorization for services covered by indiana health coverage programs (ihcp). Web prior authorization request form. Check the radio button of the entity that must authorize the service. Web covermymeds is envolve pharmacy solutions’ preferred way to receive prior authorization requests. Please refer to the procedure code lookup tool to.

Free Medicaid (Rx) Prior Authorization Forms PDF eForms
Please refer to the procedure code lookup tool to. Web prior authorization request form. The indiana health coverage programs (ihcp) requires prior authorization (pa) for certain covered. Check the radio button of the entity that must authorize the service. Prior authorization is required for certain covered services to document the medical necessity for those.

20202024 Form AR Medicaid Prior Authorization Request Fill Online, Printable, Fillable, Blank
Web prior authorization request form. (for managed care, check the. Web an indiana medicaid prior authorization form is a document used by medical professionals to request medicaid coverage for a prescription drug not. Please refer to the procedure code lookup tool to. Web covermymeds is envolve pharmacy solutions’ preferred way to receive prior authorization requests.

Fidelis medicaid prior authorization form Fill out & sign online DocHub
Please refer to the procedure code lookup tool to. Web prior authorization request form. Web an indiana medicaid prior authorization form is a document used by medical professionals to request medicaid coverage for a prescription drug not. Web this form is for providers to request prior authorization for services covered by indiana health coverage programs (ihcp). Web covermymeds is envolve.

Free Anthem Blue Cross / Blue Shield Prior Prescription (Rx) Authorization Form PDF
Web covermymeds is envolve pharmacy solutions’ preferred way to receive prior authorization requests. Web see the ihcp provider quick reference at in.gov/medicaid/providers for mailing address or fax number. Web this form is for providers to request prior authorization for services covered by indiana health coverage programs (ihcp). Web an indiana medicaid prior authorization form is a document used by medical.

Indiana Medicaid Prior Authorization Form Template and guide airSlate SignNow
Web this form is for providers to request prior authorization for services covered by indiana health coverage programs (ihcp). Web access the caresource indiana medicaid prior authorization list. Check the radio button of the entity that must authorize the service. Web prior authorization request form. Web an indiana medicaid prior authorization form is a document used by medical professionals to.

Top 17 Medicaid Prior Authorization Form Templates free to download in PDF format
Please refer to the procedure code lookup tool to. Check the radio button of the entity that must authorize the service. (for managed care, check the. Web access the caresource indiana medicaid prior authorization list. Web covermymeds is envolve pharmacy solutions’ preferred way to receive prior authorization requests.

Fillable Standard Prior Authorization Request Form United Healthcare printable pdf download
Web covermymeds is envolve pharmacy solutions’ preferred way to receive prior authorization requests. Web an indiana medicaid prior authorization form is a document used by medical professionals to request medicaid coverage for a prescription drug not. (for managed care, check the. Web access the caresource indiana medicaid prior authorization list. Web prior authorization request form.
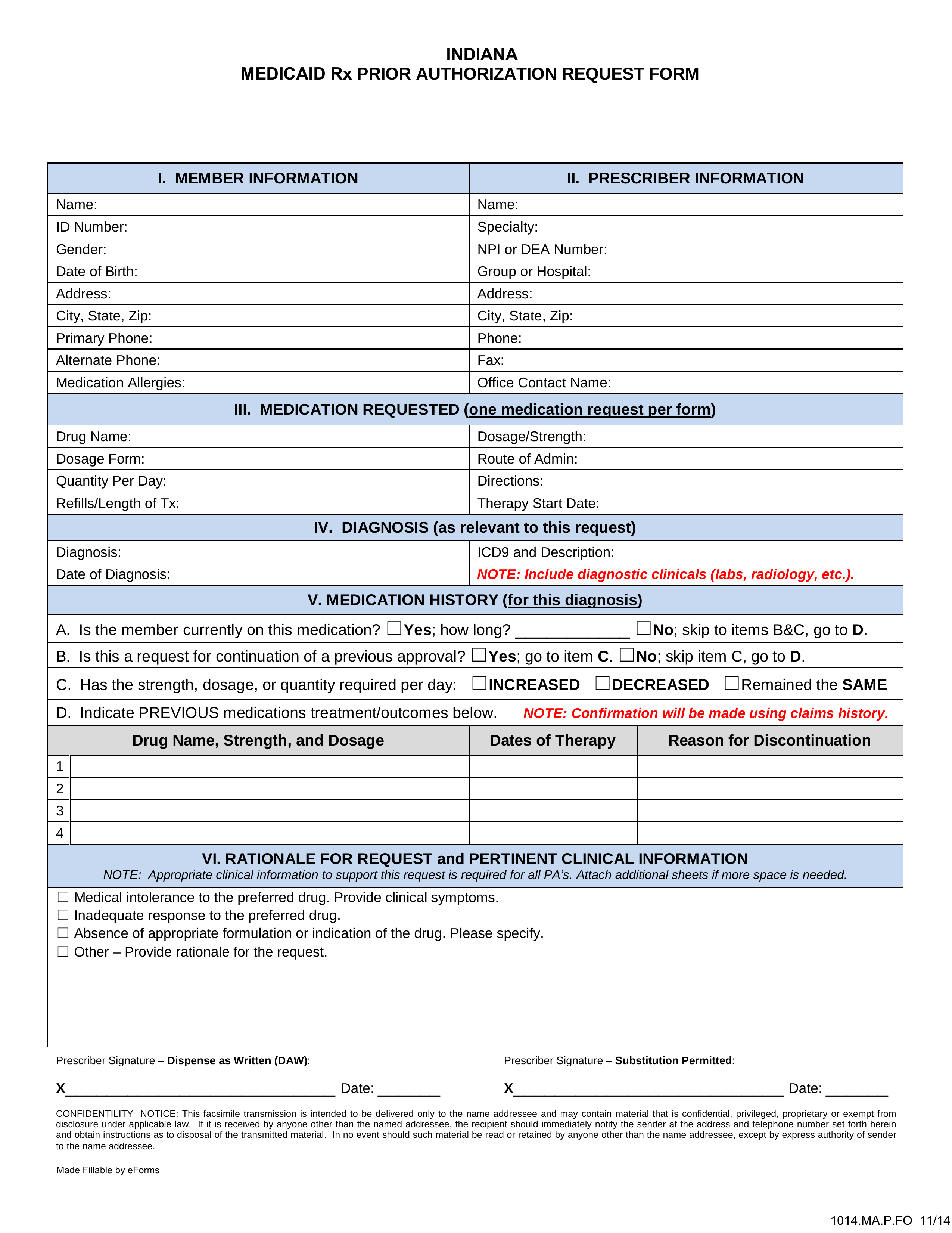
Free Indiana Medicaid Prior (Rx) Authorization Form PDF eForms
Web this form is for providers to request prior authorization for services covered by indiana health coverage programs (ihcp). Web prior authorization request form. Web see the ihcp provider quick reference at in.gov/medicaid/providers for mailing address or fax number. Web access the caresource indiana medicaid prior authorization list. Please refer to the procedure code lookup tool to.
Web see the ihcp provider quick reference at in.gov/medicaid/providers for mailing address or fax number. Please refer to the procedure code lookup tool to. The indiana health coverage programs (ihcp) requires prior authorization (pa) for certain covered. Web an indiana medicaid prior authorization form is a document used by medical professionals to request medicaid coverage for a prescription drug not. Prior authorization is required for certain covered services to document the medical necessity for those. (for managed care, check the. Web prior authorization request form. Web access the caresource indiana medicaid prior authorization list. Web covermymeds is envolve pharmacy solutions’ preferred way to receive prior authorization requests. Check the radio button of the entity that must authorize the service. Web this form is for providers to request prior authorization for services covered by indiana health coverage programs (ihcp).
Web Covermymeds Is Envolve Pharmacy Solutions’ Preferred Way To Receive Prior Authorization Requests.
The indiana health coverage programs (ihcp) requires prior authorization (pa) for certain covered. Web see the ihcp provider quick reference at in.gov/medicaid/providers for mailing address or fax number. Web access the caresource indiana medicaid prior authorization list. Web an indiana medicaid prior authorization form is a document used by medical professionals to request medicaid coverage for a prescription drug not.
(For Managed Care, Check The.
Check the radio button of the entity that must authorize the service. Web prior authorization request form. Prior authorization is required for certain covered services to document the medical necessity for those. Please refer to the procedure code lookup tool to.