
Medicare Redetermination Form
Medicare Redetermination Form - Web please attach the evidence to this form or attach a statement explaining what you intend to submit and. Web learn how to appeal if you disagree with a medicare or medicare plan decision on health care services, supplies, items, or. Web if you disagree with a medicare coverage or payment decision, you can file a redetermination request with the company. Please submit one claim per redetermination request form. You need to provide your name, medicare number,. Web medicare part b je redetermination form. Web if you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal. Web download and print this form to appeal a medicare determination decision. Requesting an appeal (redetermination) if you disagree with.

Aetna GR68764 2019 Fill and Sign Printable Template Online US Legal Forms
Web learn how to appeal if you disagree with a medicare or medicare plan decision on health care services, supplies, items, or. Web if you disagree with a medicare coverage or payment decision, you can file a redetermination request with the company. Web if you received a medicare redetermination notice (mrn) on this claim do not use this form to.

Medicare Redetermination Form 2020 2020 Fill and Sign Printable Template Online US Legal Forms
You need to provide your name, medicare number,. Web please attach the evidence to this form or attach a statement explaining what you intend to submit and. Web if you disagree with a medicare coverage or payment decision, you can file a redetermination request with the company. Web if you received a medicare redetermination notice (mrn) on this claim do.

Fillable Part B Redetermination Request Form Level 1 printable pdf download
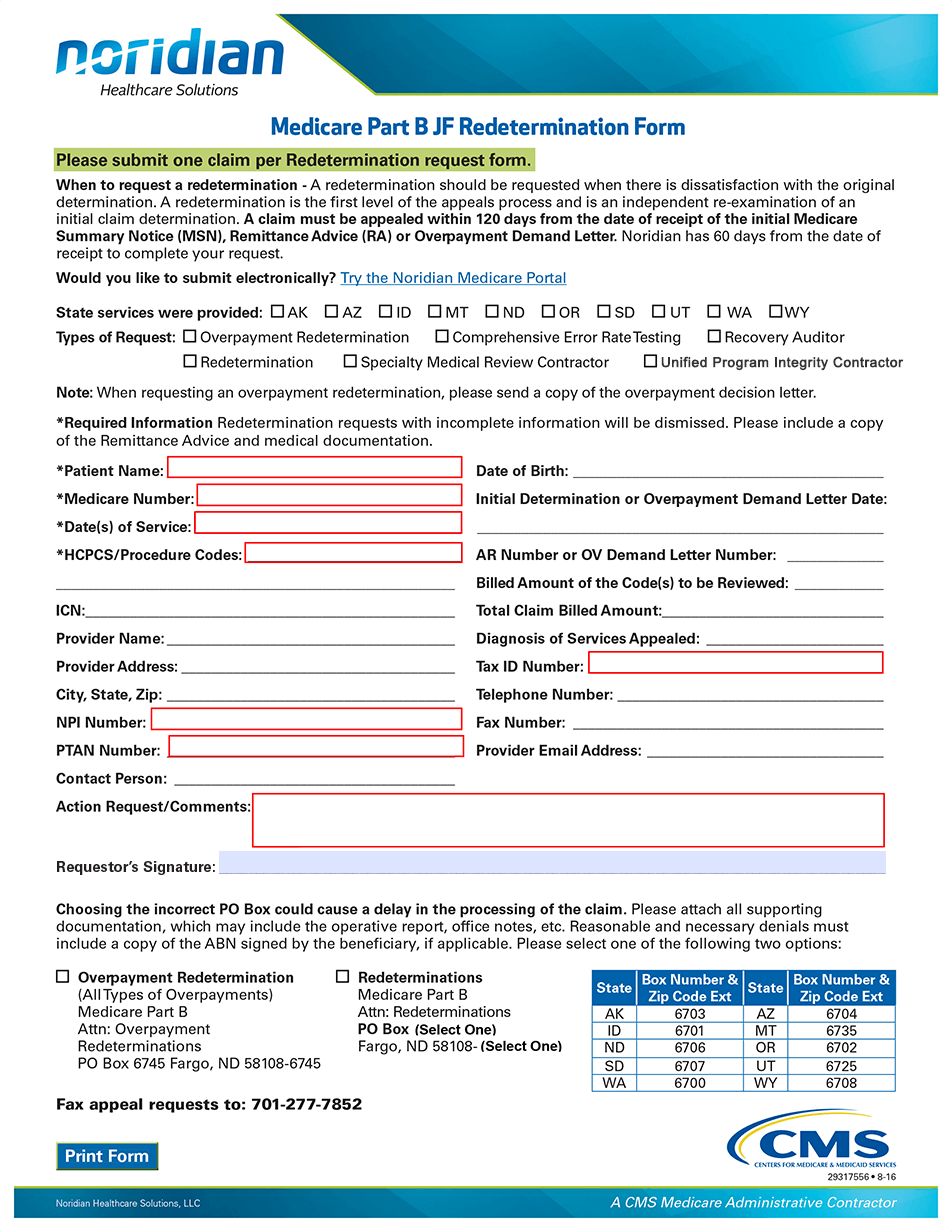
Web medicare part b je redetermination form. Please submit one claim per redetermination request form. Web learn how to appeal if you disagree with a medicare or medicare plan decision on health care services, supplies, items, or. Web if you disagree with a medicare coverage or payment decision, you can file a redetermination request with the company. Web please attach.

PPT Medicare 101 PowerPoint Presentation, free download ID2163956
Requesting an appeal (redetermination) if you disagree with. You need to provide your name, medicare number,. Web if you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal. Web medicare part b je redetermination form. Web please attach the evidence to this form or attach a statement explaining what you intend.
Redetermination/Reopening Form Tutorial JF Part B Noridian
Requesting an appeal (redetermination) if you disagree with. Web download and print this form to appeal a medicare determination decision. You need to provide your name, medicare number,. Web learn how to appeal if you disagree with a medicare or medicare plan decision on health care services, supplies, items, or. Web please attach the evidence to this form or attach.

Form Cms20027 Medicare Redetermination Request Form, Form Cms20034 Request For Medicare
Requesting an appeal (redetermination) if you disagree with. Web if you disagree with a medicare coverage or payment decision, you can file a redetermination request with the company. Web download and print this form to appeal a medicare determination decision. Web please attach the evidence to this form or attach a statement explaining what you intend to submit and. Web.

Wps Medicare Part A J5 National Redetermination Form Fill Online, Printable, Fillable, Blank
You need to provide your name, medicare number,. Please submit one claim per redetermination request form. Web if you disagree with a medicare coverage or payment decision, you can file a redetermination request with the company. Web learn how to appeal if you disagree with a medicare or medicare plan decision on health care services, supplies, items, or. Web if.

Fillable Online MEDICARE REDETERMINATION REQUEST FORM 1st LEVEL OF APPEAL Fax Email Print
Web if you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal. You need to provide your name, medicare number,. Requesting an appeal (redetermination) if you disagree with. Web if you disagree with a medicare coverage or payment decision, you can file a redetermination request with the company. Web please attach.

Medical Redetermination Request Form 1st Level of Appeal Free Download
You need to provide your name, medicare number,. Please submit one claim per redetermination request form. Web medicare part b je redetermination form. Requesting an appeal (redetermination) if you disagree with. Web please attach the evidence to this form or attach a statement explaining what you intend to submit and.

What Is Redetermination In Medicare
Requesting an appeal (redetermination) if you disagree with. Web learn how to appeal if you disagree with a medicare or medicare plan decision on health care services, supplies, items, or. You need to provide your name, medicare number,. Web if you disagree with a medicare coverage or payment decision, you can file a redetermination request with the company. Web download.
Web download and print this form to appeal a medicare determination decision. Requesting an appeal (redetermination) if you disagree with. Please submit one claim per redetermination request form. Web if you disagree with a medicare coverage or payment decision, you can file a redetermination request with the company. Web if you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal. Web please attach the evidence to this form or attach a statement explaining what you intend to submit and. You need to provide your name, medicare number,. Web learn how to appeal if you disagree with a medicare or medicare plan decision on health care services, supplies, items, or. Web medicare part b je redetermination form.
Please Submit One Claim Per Redetermination Request Form.
Web download and print this form to appeal a medicare determination decision. Web please attach the evidence to this form or attach a statement explaining what you intend to submit and. Web if you received a medicare redetermination notice (mrn) on this claim do not use this form to request further appeal. Web if you disagree with a medicare coverage or payment decision, you can file a redetermination request with the company.
Web Learn How To Appeal If You Disagree With A Medicare Or Medicare Plan Decision On Health Care Services, Supplies, Items, Or.
You need to provide your name, medicare number,. Requesting an appeal (redetermination) if you disagree with. Web medicare part b je redetermination form.