
Molina Appeals Form
Molina Appeals Form - Web if you don’t agree with the decision molina healthcare (molina) has made on a service request or payment issue, you have the. Please submit the request by our preferred method, visiting the provider portal,. Web to make an appeal, you must contact molina within 60 calendar days of the denial. Web this form can be used for up to 9 claims that have the same denial reason. Web member grievance/appeal request form. Web provider claim appeal and dispute form. If you have 10 or more claims,. Please include a copy of the eob with the appeal and any supporting documentation. Call the california state department of managed health care. Web claim reconsideration request form.

Fillable Online Provider Claim Appeal and Dispute Form Molina Healthcare Fax Email Print
Web this form can be used for up to 9 claims that have the same denial reason. Please submit the request by our preferred method, visiting the provider portal,. Web member grievance/appeal request form. Web claim reconsideration request form. Web if you don’t agree with the decision molina healthcare (molina) has made on a service request or payment issue, you.

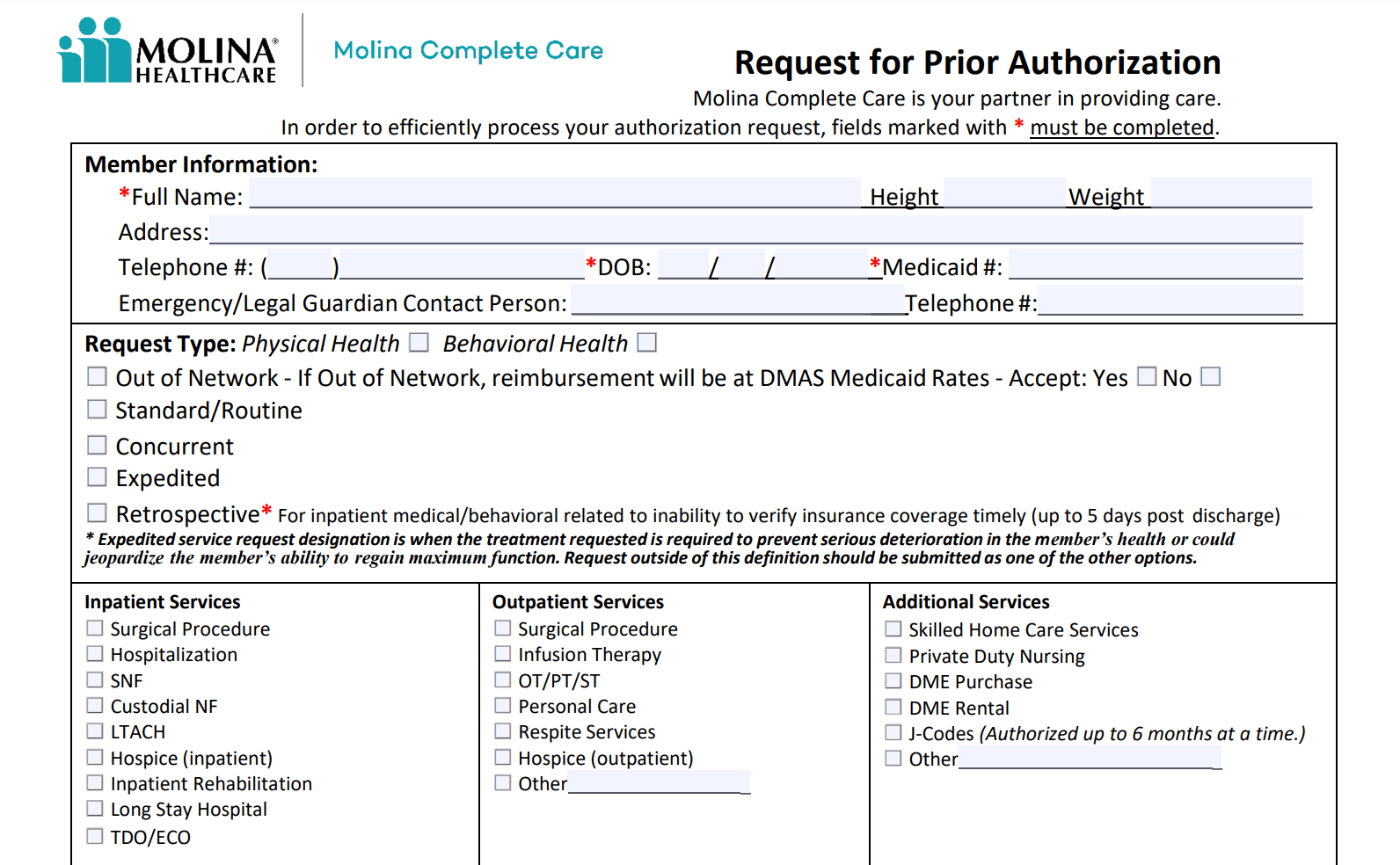
Molina Healthcare Prior Authorization Service Request Form
Web if you don’t agree with the decision molina healthcare (molina) has made on a service request or payment issue, you have the. Please include a copy of the eob with the appeal and any supporting documentation. Call the california state department of managed health care. Please submit the request by our preferred method, visiting the provider portal,. Web claim.
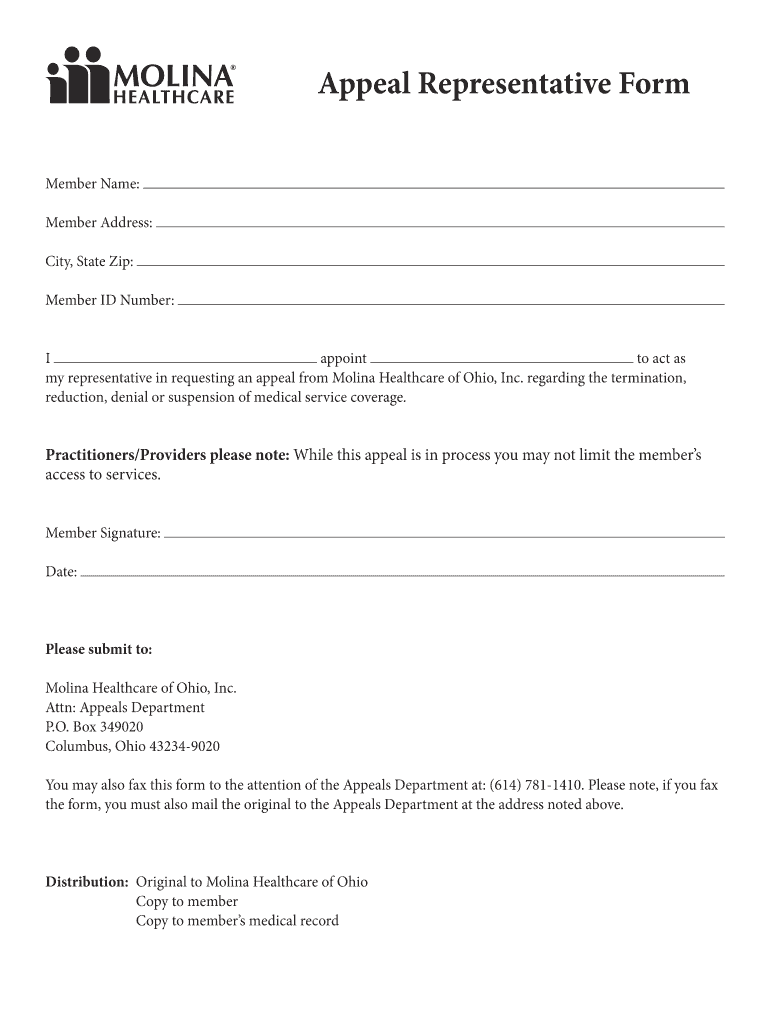
Fillable Online Molina appealrepform. Molina appealrepform Fax Email Print pdfFiller
Web if you don’t agree with the decision molina healthcare (molina) has made on a service request or payment issue, you have the. Please include a copy of the eob with the appeal and any supporting documentation. Web member grievance/appeal request form. Web provider claim appeal and dispute form. Please submit the request by our preferred method, visiting the provider.

Free Molina Healthcare Prior (Rx) Authorization Form PDF eForms
Web member grievance/appeal request form. Web claim reconsideration request form. Please submit the request by our preferred method, visiting the provider portal,. Web if you don’t agree with the decision molina healthcare (molina) has made on a service request or payment issue, you have the. Web this form can be used for up to 9 claims that have the same.

Molina Medicare Pa Forms Universal Network
Call the california state department of managed health care. Web if you don’t agree with the decision molina healthcare (molina) has made on a service request or payment issue, you have the. If you have 10 or more claims,. Please include a copy of the eob with the appeal and any supporting documentation. Web claim reconsideration request form.

Molina appeal form Fill out & sign online DocHub
Web if you don’t agree with the decision molina healthcare (molina) has made on a service request or payment issue, you have the. Web to make an appeal, you must contact molina within 60 calendar days of the denial. Please include a copy of the eob with the appeal and any supporting documentation. Web claim reconsideration request form. Call the.
Doing a PreCertification or Prior Authorization with Molina HealthCare for Addiction Treatment
If you have 10 or more claims,. Please include a copy of the eob with the appeal and any supporting documentation. Call the california state department of managed health care. Please submit the request by our preferred method, visiting the provider portal,. Web if you don’t agree with the decision molina healthcare (molina) has made on a service request or.

Molina Healthcare Medicaid And Medicare Prior Authorization Request Form printable pdf download
Please submit the request by our preferred method, visiting the provider portal,. Web this form can be used for up to 9 claims that have the same denial reason. Web provider claim appeal and dispute form. Web claim reconsideration request form. Call the california state department of managed health care.

Molina Provider Form Ny Fill Online, Printable, Fillable, Blank pdfFiller
Web member grievance/appeal request form. Call the california state department of managed health care. Web this form can be used for up to 9 claims that have the same denial reason. Please include a copy of the eob with the appeal and any supporting documentation. Please submit the request by our preferred method, visiting the provider portal,.

Fillable Online Molina Healthcare Member Grievance/Appeal Request Form Fax Email Print
Web provider claim appeal and dispute form. Web to make an appeal, you must contact molina within 60 calendar days of the denial. Web if you don’t agree with the decision molina healthcare (molina) has made on a service request or payment issue, you have the. Call the california state department of managed health care. If you have 10 or.
Please submit the request by our preferred method, visiting the provider portal,. If you have 10 or more claims,. Please include a copy of the eob with the appeal and any supporting documentation. Web this form can be used for up to 9 claims that have the same denial reason. Web claim reconsideration request form. Web provider claim appeal and dispute form. Call the california state department of managed health care. Web if you don’t agree with the decision molina healthcare (molina) has made on a service request or payment issue, you have the. Web to make an appeal, you must contact molina within 60 calendar days of the denial. Web member grievance/appeal request form.
Web Member Grievance/Appeal Request Form.
Web to make an appeal, you must contact molina within 60 calendar days of the denial. Web provider claim appeal and dispute form. Please include a copy of the eob with the appeal and any supporting documentation. Web this form can be used for up to 9 claims that have the same denial reason.
Web If You Don’t Agree With The Decision Molina Healthcare (Molina) Has Made On A Service Request Or Payment Issue, You Have The.
If you have 10 or more claims,. Please submit the request by our preferred method, visiting the provider portal,. Web claim reconsideration request form. Call the california state department of managed health care.